


“I felt the blast from a terrific explosion which had occurred somewhere behind me. The blast was such that it threw me full length across the road. Debris then began to fall all around me, and I was covered with oil which fell out of the sky,” a worker at the Flixborough Works of Nypro Limited chemical plant told investigators about the explosion there at seven minutes before 5:00 pm on June 1st, 1974.
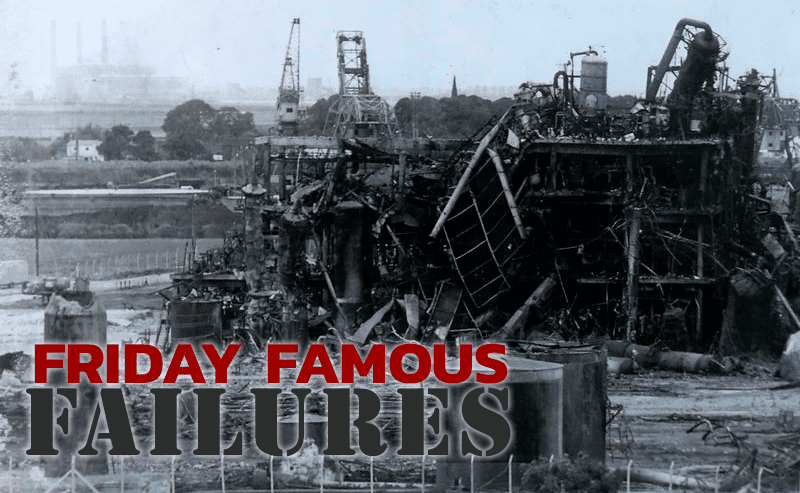
The explosion at the chemical plant, which was situated on the banks of the River Trent in Lincolnshire, was the biggest explosion to ever occur in Britain (during peacetime) until the fire at the Hertfordshire oil storage terminal (Buncefield) in December 2005. Twenty-eight of Flixborough Nypro’s 550 workers were killed, and 36 others onsite were injured, as the explosion destroyed the plant and sent debris raining down on Hull and its surrounding area.
Outside the plant, injuries and damage occurred on a widespread scale, but there were no fatalities. The number of casualties would have been even higher had the incident occurred on a weekday. In total, the explosion, estimated to be equivalent to 16 metric tons of TNT, caused damage to 1,821 nearby houses and 167 shops and factories and was heard over 30 miles away in Grimsby. The fire from the explosion burned for 10 straight days. At the height of the incident, 49 firefighting vehicles were in attendance.
Flixborough Nypro had been designed to produce 70,000 metric tons per year of caprolactam, a raw material used in the creation of Nylon 6, a plastic used to manufacture clothing, carpets, fishing nets, ropes, and belts. Nypro’s caprolactam unit performed cyclohexane oxidation in a series of six successive reactors. Difficulties arose at the end of March 1974 when one of the valves on Reactor 5 was found to be in bad shape and had to be kept cool by spraying it with water. The nitrate in the water, plus the heat of the reactor vessel, resulted in stress cracking of the vessel wall. By the next day, this detected crack was already extending a full two meters in length. Reactor 5 was removed for inspection.
In order to resume production as quickly as possible, plant engineers built a bypass between Reactors 4 and 6, specifically between their 28-inch diameter expansion fans, and implemented it without any specific preliminary study, based solely on a drawing produced on the shop floor. The feed pipes that connected the reactors were supposed to be 28 inches in diameter, but because of elevation changes, it was necessary to incorporate a “dogleg” in this piping jumper, using 20-inch diameter pipe (the only pipe available on site) supported by scaffolding. The temporary modification was not assessed or pressure tested prior to installation.
It should be noted that at the beginning of 1974 the maintenance engineer left the factory for personal reasons, and by June 1974 the company had not yet found a replacement. None of the other engineers had special competence in mechanical engineering.
At 4:53 pm on June 1st, a subsonic combustion noticeable up to three miles away practically leveled the entire site. In many sectors of the plant, intense fires ensued, with flames flaring 230 to 328 feet high. The main sources of ignition would not be extinguished until two and a half days later. The massive explosion killed 18 people who were in the control room at the time. Thirty-six more were injured.
What exactly had caused the explosion and fire at Flixborough Works of Nypro?
The Investigation and Causal Factors of the Explosion
The official Commission of Enquiry (also referred to as the Court of Inquiry) launched a 70-day investigation into the Flixborough explosion—the longest of its kind ever held in the UK. The disaster was the culmination of a chain of consequences, starting with a massive stress corrosion crack in Reactor 5. The cause of the accident was believed to have been directly associated with the design and installation of the temporary pipe that had been installed as a connector between Reactors 4 and 6 after Reactor 5 had been removed.
But other failures also contributed to the disaster: a number of mechanical failures were overlooked by managers prior to the explosion, and the plant had no onsite personnel with the correct knowledge and qualifications to make the repairs that had been hastily made.
Investigators determined that the most likely source of the cyclohexane release was the “dogleg” piping jumper that had been retrofitted to connect Reactor 4 to Reactor 6. It is believed that the unbalanced forces imposed on the bends in the piping, coupled with the flexibility introduced by the expansion bellows, allowed the inadequately supported and unconstrained jumper to oscillate. Ultimately, one of the bellows failed, releasing the process fluid.
The official report into the explosion revealed 12 causal factors of the disaster:
- No mechanical engineers on staff. After the early 1974 departure of the maintenance engineer, the company had not yet found a replacement by the date of the disaster. None of the other engineers had special competence in mechanics.
- Lack of inspection. Even though a significant crack was found in Reactor 5, the decision was made to restart the process without inspecting the other reactors to determine if similar cracks existed.
- Staff treated the bypass as a routine plumbing task. Staff involved in planning and implementing the bypass approached the task as if it were a routine plumbing task.
- The urgency to resume production distracted staff from critical consideration of their plans that could have identified the hazards involved.
- Short staffing affected facility performance. The fact that the works manager position was vacant shifted workload to remaining staff, which contributed to the distractions. Company management was not aware of the effect of the short staffing on the performance of the facility staff involved in the modification.
- No consideration given to bending and thrusting in the dogleg configuration. While calculations were made to confirm that the 20-inch pipe could withstand the normal working pressure, no consideration was given to the bending moments or hydraulic thrusts that would be imposed due to its dogleg configuration.
- No consideration given to torque reaction on the fans. No one gave thought to the fact that the whole installation, once pressurized, would be subject to a torque reaction that would shear the fans, which had not been designed for this, nor did anyone take into account the fact that the strong hydraulic pressure on the fans would tend to buckle the bypass at the joints.
- Manufacturer guidelines were not followed. No reference was made to the user guidelines published by the manufacturer of the fans.
- Lack of dogleg piping layout and design. No drawing was made for the piping layout and design, other than a chalk sketch made on the floor of the maintenance workshop.
- Lack of piping support. No pillar or other means was used either to support the piping from underneath or to prevent lateral movement.
- Lack of quality assurance. There were no quality assurance checks made on the 20-inch pipe/dogleg or its installation other than a leak check at approximately 130 psi.
- Lack of safety policies and procedures. Nypro did not have an adequate system for evaluating and controlling changes to ensure that safety was not impacted.
The After-Effects of the Disaster
The Flixborough explosion strongly shook the British population and rattled the confidence of every chemical engineer in the country. In a perfectly-clear manner, it demonstrated the necessity to postulate the possibility of a massive escape of gas and the formation of clouds from containers holding inflammable liquids kept under pressure and at temperatures above their boiling point.
The explosion led to a public outcry over process safety. The passage of the Health and Safety Act later that year enacted a standardized system of safety procedures to prevent incidents like this from being repeated. This incident highlights the importance of having a trained and competent workforce. Changes in work processes must be well planned by employees who possess suitable knowledge and training.
Flixborough gave the world 10 safety lessons it still heeds today:
- The death of 19 people in the control room demonstrates the necessity to carefully design the layout and location of control rooms so as to mitigate the risks borne by personnel inside the facility.
- The placement of administrative buildings, laboratories, etc., must be studied in depth to isolate the most hazardous units and limit their access to just authorized staff.
- One of the means available for reducing the risk of major accidents is to limit hazard potential, specifically through lowering the quantities of hazardous materials that are stored onsite.
- The design, construction, and control of modifications for hazardous installations must be undertaken according to the same standards as the original facility since any modification, no matter how small, can engender risk.
- Temporary repair work is never justified, and this requires even more emphasis when the repair tends to become definitive.
- Beyond reducing risks strictly related to physical deficiencies, an organized and planned preventive maintenance program is always preferable to any kind of emergency intervention.
- Resuming installation operations after an incident requires a preliminary analysis of the causes leading to the shutdown.
- Critical safety specifications must not be overlooked, especially in the presence of a high-hazard potential.
- Any intervention procedure needs first to be examined and its consequences assessed prior to adoption since an ill-suited intervention could give rise to risk.
- Only a well-skilled and experienced workforce would be able to recognize precursor signals of an accident (such as cyclohexane leaks that “seal up on their own”) and to adopt necessary measures to halt the accidental sequence. A well-trained staff proves essential to introducing a safety program for a hazardous installation.

I would suspect that inadequate spacing between certain hazardous equipment was a contributing factor. Plus, inadequate fire protection in terms of quantity and pressure of fire protection water for monitors and spray systems. The plant should have been reduced to minimum product production and, better yet, shutdown for correct repairs and to take care of other worn or unsafe equipment, piping, and supports, etc.
Greg Harrison, PhD., P.E.
Fire Protection & Civil Engineer